Cart (0)
Subtotal
0,00 €

By: Nature Going Smart Activism
cannabis is often compared to alcohol or cigarettes in various articles, studies and campaigns. Alcohol and cigarettes are more familiar to the average person than cannabis and comparing something that is legal, and generally not good for your health, to something that is illegal and generally good for your health, makes sense. Or does it?
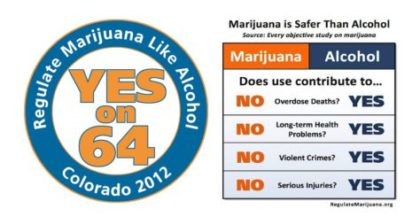
Comparing cannabis and alcohol was one of the ways the Amendment 64 was successfully passed in 2012, making Colorado the first state to legalize cannabis in USA (1). Some of the arguments that they used were:

Can we really compare these three? In this article, I will try to give you an insight to what the studies and science has to say about these three substances.
When we talk about addiction and the addictive properties of certain drugs, we must first understand what addiction really means.
One of the best explanations that I heard was from Dr. Mate Gabor, a world-renowned expert in addiction. He summarizes addiction in this short video:
In the short clip, Dr. Mate mentioned the CDC-Kaiser Permanente Adverse Childhood Experiences (ACE) Study.
This is one of the largest investigations of childhood abuse and neglect and later-life health and well-being. Specific studies have been done on ACE’s correlation with alcohol (3-7), drugs (8) and smoking (9-12).
Understanding this concept is essential for interpreting various number that are given regarding addiction to these substances.
Some studies estimate the probability of transition to cannabis dependence being 8,9%, which is lower than alcohol 22,7% and cigarettes 67,5% (13). It is interesting to note, that cannabis is often successfully used to get off other more addictive substances like nicotine (14), alcohol (15-19), cocaine (20, 21), opioids and other prescription drugs (15-18 ).
Smoking and alcohol both pose a risk to one’s health, if they are consumed regularly. Alcohol has a negative impact on many body organs (brain, heart, liver and pancreas) and the immune system. Smoking cigarettes is also very deleterious on your body:
“Cigarette smoking harms nearly every organ of the body, causes many diseases, and reduces the health of smokers in general.” CDC
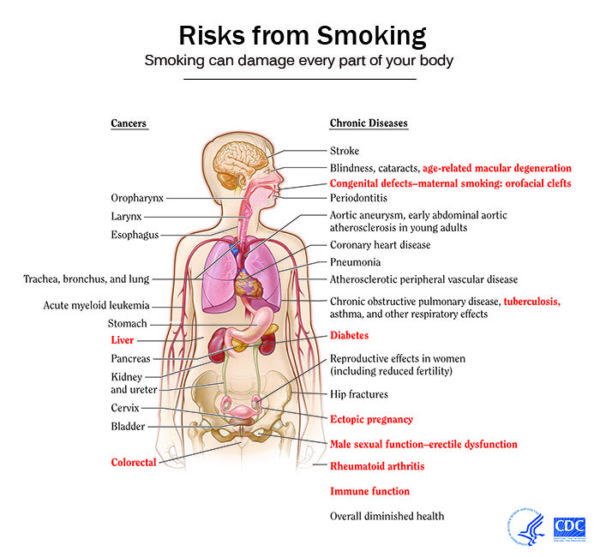
Smoking is a leading cause of cancer and death from cancer. Smoking causes heart disease, stroke, aortic aneurysm (a balloon-like bulge in an artery in the chest), chronic obstructive pulmonary disease (COPD) (chronic bronchitis and emphysema), diabetes, osteoporosis, rheumatoid arthritis, age-related macular degeneration, and cataracts, and worsens asthma symptoms in adults. Smokers are at higher risk of developing pneumonia, tuberculosis, and other airway infections. In addition, smoking causes inflammation and impairs immune function.
National cancer institute
It is interesting to note, that cannabis and cannabinoids have been shown to have a beneficial impact on all of the negative effects and diseases caused by alcohol and smoking, and you can read more by saving these articles for later “Cannabis & cancer“, “Cannabis & diabetes” .
Below I will focus and compare three health issues and that are common to all of the mentioned substances.
Smoking can cause cancer almost anywhere in the body and increases the risk of dying from other diseases in cancer patients and survivors (22). Organs that are exposed to smoke are more susceptible to becoming cancerous (esophagus, larynx, oropharynx, esophagus trachea, bronchus, and lungs) but also other organs can be targeted (liver, pancreas, stomach, kidney, ureter, blood, bladder, cervix, colon and rectum)(23).
Drinking alcohol can also increase the risk of developing certain cancers, mainly cancers of the mouth, throat, esophagus, liver and breast (24).
Based on extensive reviews of research studies, there is a strong scientific consensus of an association between alcohol drinking and several types of cancer. In its Report on Carcinogens, the National Toxicology Program of the US Department of Health and Human Services lists consumption of alcoholic beverages as a known human carcinogen. (25)
Studies done on cell cultures (in vitro) and on animals (in vivo) have shown that pyhtocannabinoids (found in cannabis), but also endogenous and synthetic cannabinoids, are capable of effectively decreasing tumor growth and invasion in many types of cancers. Discover more on CBD & metastasis (26). Sadly, there is a lack of clinical trials on humans, but there are numerous anecdotal testimonials of people, who have successfully treated their cancer with various cannabis preparations (27).
Smokers are at greater risk for cardiovascular diseases. Smoking damages the blood vessels, makes them thicker and narrower (peripheral arterial disease). This rises the blood pressure and can form clots that can block the flow of blood (ischaemic stroke) or burst the blood vessel (haemorrhagic stroke).
Did you know that Yoga could be a great tool for prevention & treatment of hypertension? Check out more here!
Smoking can also affect the heart and can cause the enlargement of the abdominal aorta (abdominal aortic aneurysm) (30, 32).
Cigarette smoke includes more than 4,000 chemical substances, including polycyclic aromatic hydrocarbons and oxidative gases, most of which exert a cardiotoxic effect. (31)
Alcohol consumption and abuse has been found to increase the risk of heart attack (myocardial infarction) heart failure (congestive heart failure) and atrial fibrillation (abnormal heart rhythm characterized by rapid and irregular beating) (28). You can often hear that moderate alcohol consumption, especially red wine, can be cardio protective, but the evidence from randomized clinical trials suggests that it is not relevant (29).
The recent infatuation with the potential benefits of light-to-moderate drinking for cardiovascular disease protection appears to be based on observational and subtly confounded data, rather than on randomized clinical trials evidence, and perhaps on more than a little wishful thinking. (29)
Generally speaking, cannabinoid type 1 receptor (CB1) activation has undesired effects on the cardiovascular system while cannabinoid type 2 receptor (CB2) activation has a cardio-protective role. There have been studies suggesting that cannabis use can increase the chance of having a heart attack (36-39) however, longitudinal studies have shown no relationship between cannabis use, heart attacks and cardio vascular diseases (40-42).
If you don’t know what CB1 & CB2 are, and what the Endocannabinoid System is, I recommend you read this introduction “Understanding the Endocannabinoid System”
THC activates (partial agonist) both CB1 and CB2 receptors, which does not make it an ideal cannabinoid for cardio protection. It can increase heart rate (tachycardia), increase or lower the blood pressure and it can sometimes cause a sudden fall of blood pressure when suddenly standing up from a lying or sitting position (orthostatic hypotension). On the other hand, in animal studies, THC has also been shown to protect heart cells from lack of oxygen and prevent the progression of atherosclerosis (34, 35).
Cannabidiol (CBD) has shown very positive results (in vivo and in vitro) in preventing cardiac complications and symptoms in diabetes related heart muscle disorder (diabetic cardiomyopathy), reducing vascular inflammation, reducing infarct related cell death and being neuroprotective in strokes (43-52).
Another promising cannabinoid for cardiovascular diseases is THC’s little brother tetrahydrocannabivarin (THCV). It activates the CB2 receptor and blocks the CB1 receptor, which makes it a good candidate for the prevention of negative symptoms from diabetes and metabolic syndrome (53).
There are many factors that can influence ones sexual life. Many disease, such as rheumatic disease (54), diabetes(55) and PTSD (56), and drugs such as opioids (59-61) have been shown to have a negative impact on sexual functioning.
Both alcohol and cigarettes have been linked to sexual dysfunctions, such as difficulty in erection and decreased sexual desire (58). These effects are more pronounced in heavy smokers and heavy drinkers
Episodic erectile failure in alcoholic men is fairly routine, found to be significantly higher in men consuming more than three standard units of alcohol (12 g ethanol) daily and in subjects smoking more than 10 cigarettes/day. (57)
Many studies have shown that cigarette smokers, especially heavy smoking, have a higher risk of having impotence and decrease sexual desire (62-78)
The endocannabinoid system (ECS) is heavily involved in the human (mammalian) reproductive system, modulating several important aspects of the reproductive cycle, as I have described in this other article: “Endocannabinoids: co-creators of life” .
Many complications, which some couples have with getting pregnant, might be linked, to incorrect working of the ECS. Clinical trials on humans, investigating the effects of cannabis, are missing and most of the data is from old studies. Most users report a dose-dependent beneficial effect on sexual function, reporting increases in sexual desire, sensuality, pleasure, length of intercourse and number of orgasms (79).
Recent studies have shown cannabis use increases activity of brain areas (right nucleus accumbens) responsive to visual erotica stimuli. This could be a novel treatment for people with low sexual desire (80).
Check out other holistic ways to improve fertility, and this insight on Yoga to treat sexual dysfunction in man as well as for both in the couple.
Worldwide, tobacco use causes nearly 6 million deaths per year (480,000 deaths per year in the USA alone, including more than 41,000 deaths resulting from secondhand smoke exposure) and 3.3 million people die from alcohol-related causes (88,000 deaths in the USA) (81-83).
There has not been a documented case of death due to cannabis (84). Ever.
Just by comparing these facts, one comes to the conclusion, that cannabis should not be compared to these other substances. While THC, the most abundant cannabinoid in most chemovars, does have some unwanted side effects, these can be successfully mitigated by other cannabinoids (CBD, THCV) and terpenes (alpha-pinene, D-limonene), changing methods of consumption (vaporizing vs. smoking) and adequate dosing regimens (micro-dosing, building tolerance).
It is probably still one of the safest active therapeutic substances known to man (85).
1 Joshua Kappel. Legalized it. The beginning of the end of Cannabis Prohibition in the U.S.A.
2 Campaign to Regulate Marijuana Like Alcohol Issues Statement Regarding the Narrow Defeat of Prop. 205 https://www.regulatemarijuanainarizona.org/campaign-regulate-marijuana-l…
3 Anda RF, Whitfield CL, Felitti VJ, Chapman D, Edwards VJ, Dube SR, Williamson DF. Adverse childhood experiences, alcoholic parents, and later risk of alcoholism and depression. Psychiatr Serv. 2002;53(8):1001–1009.
4 Dube SR, Anda RF, Felitti VJ, Croft JB, Edwards VJ, Giles WH. Growing up with parental alcohol abuse: exposure to childhood abuse, neglect and household dysfunction. Child Abuse and Negl. 2001;25(12):1627–1640.
5 Dube SR, Anda RF, Felitti VJ, Edwards VJ, Croft JB. Adverse Childhood Experiences and personal alcohol abuse as an adult. Addictive Behaviors. 2002;27(5):713–725.
6 Dube SR, Miller JW, Brown DW, Giles WH, Felitti VJ, Dong M, Anda RF. Adverse childhood experiences and the association with ever using alcohol and initiating alcohol use during adolescence. J Adolesc Health. 2006;38(4):444.e1-444.e10.
7 Strine TW, Dube SR, Edwards VJ, Prehn AW, Rasmussen S, Wagenfeld M, Dhingra S, Croft JB. Associations between adverse childhood experiences, psychological distress, and adult alcohol problems. Am J Health Behav. 2012 Mar; 36(3):408-23.
8 Dube SR, Felitti VJ, Dong M, Chapman DP, Giles WH, Anda RF. Childhood abuse, neglect and household dysfunction and the risk of illicit drug use: The Adverse Childhood Experience Study. Pediatrics. 2003;111(3):564–572.
9 Anda RF, Croft JB, Felitti VJ, Nordenberg D, Giles WH, Williamson DF, Giovino GA. Adverse childhood experiences and smoking during adolescence and adulthood. JAMA. 1999;282:1652–1658.
10 Edwards VJ, Anda RF, Gu D, Dube SR, Felitti VJ. Adverse childhood experiences and smoking persistence in adults with smoking-related symptoms and illness. Perm J. 2007;11:5–7.
11 Ford ES, Anda RF, Edwards VJ, Perry GS, Zhao G, Tsai J, Li C, Croft JB. Adverse childhood experiences and smoking status in five states. Prev Med. 2011;53:188-93.
12 Strine TW, Edwards VK, Dube SR, Wagenfeld M, Dhingra S, Prehn AW, Rasmussen S, Mcknight-Eily L, Croft JB. The mediating sex-specific effect of psychological distress on the relationship between adverse childhood experiences and current smoking among adults. Subst Abuse Treat Prev Policy. 2012;7:30.
13 Lopez-Quintero C, de los Cobos JP, Hasin DS, et al. Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: Results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug and alcohol dependence. 2011;115(1-2):120-130.
14 Celia J.A. Morgan, , Ravi K. Das, Alyssa Joye, H. Valerie Curran, Sunjeev K. Kamboj. Cannabidiol reduces cigarette consumption in tobacco smokers: Preliminary findings. Addictive Behaviors, Volume 38, Issue 9, September 2013, Pages 2433–2436
15 Zach Walsh, Raul Gonzalez, Kim Crosby, Michelle S. Thiessen, Chris Carroll, Marcel O. Bonn-Miller. Medical cannabis and mental health: A guided systematic review. Clinical Psychology Review, 2017; 51: 15
16 Brian J Piper, Rebecca M DeKeuster, Monica L Beals, Catherine M Cobb, Corey A Burchman, Leah Perkinson, Shayne T Lynn, Stephanie D Nichols, Alexander T Abess. Substitution of medical cannabis for pharmaceutical agents for pain, anxiety, and sleep. Journal of Psychopharmacology, Vol 31, Issue 5, pp. 569 – 575
17 Reiman A. Cannabis as a substitute for alcohol and other drugs. Harm Reduct. (2009) J 6: 35
18 Lucas P, Walsh Z, Crosby K, . (2016) Substituting cannabis for prescription drugs, alcohol and other substances among medical cannabis patients: The impact of contextual factors. Drug Alcohol Rev 35: 326–333.
19 Subbaraman MS. Can cannabis be considered a substitute medication for alcohol? Alcohol and Alcoholism, 2014, 49: 292–298
20 Fischer, Benedikt et al. Addressing the stimulant treatment gap: A call to investigate the therapeutic benefits potential of cannabinoids for crack-cocaine use.International Journal of Drug Policy , Volume 26 , Issue 12 , 1177 – 1182
21 M. Eugenia Socíasa, b, Thomas Kerra, b, Evan Wooda, b, Huiru Donga, Stephanie Lakea, Kanna Hayashia, b, Kora DeBecka, c, Didier Jutras-Aswadd, e, Julio Montanera, b, M.-J. Milloy. Intentional cannabis use to reduce crack cocaine use in a Canadian setting: A longitudinal analysis. Addictive Behaviors, Volume 72, September 2017, Pages 138–143
22 U.S. Department of Health and Human Services.The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014.
23 U.S. Department of Health and Human Services. How Tobacco Smoke Causes Disease: What It Means to You. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2010.
24 Alcohol’s Effects on the Body. National Institute on Alcohol Abuse and Alcoholism (NIAAA) https://www.niaaa.nih.gov/alcohol-health/alcohols-effects-body
25 Alcohol and Cancer Risk. National Cancer Institute https://www.cancer.gov/about-cancer/causes-prevention/risk/alcohol/alcoh…
26 Ladin DA, Soliman E, Griffin L and Van Dross R (2016) Preclinical and Clinical Assessment of Cannabinoids as Anti-Cancer Agents. Front. Pharmacol. 7:361.
27 Justin Kander. Cannabis for the treatment of cancer
28 Isaac R. Whitman, Vratika Agarwal, Gregory Nah, Jonathan W. Dukes, Eric Vittinghoff, Thomas A. Dewland, Gregory M. Marcus. Alcohol Abuse and Cardiac Disease. Journal of the American College of Cardiology Jan 2017, 69 (1) 13-24
29 Michael H. Criqui, Isac C. Thomas. Alcohol Consumption and Cardiac Disease: Where Are We Now? Journal of the American College of Cardiology, Volume 69, Issue 1, 3–10 January 2017, Pages 25-27
30 Villablanca, Amparo C. et al. Smoking and cardiovascular disease. Clinics in Chest Medicine , Volume 21 , Issue 1 , 159 – 172
31 Haustein K. Tobacco or Health: Physiological and Social Damages Caused by Tobacco Smoking. Berlin, Germany:Springer; 2002.
32 Vlassis N. Pyrgakis. Smoking and Cardiovascular Disease. Hellenic J Cardiol 2009; 50: 231-234
33 Christopher A. Franz; William H. Frishman. Marijuana Use and Cardiovascular Disease. Cardiology in Review. 24(4):158–162
34 Shmist YA, Goncharov I, Eichler M, et al. Delta-9-tetrahydrocannabinol protects cardiac cells from hypoxia via CB2 receptor activation and nitric oxide production. Mol Cell Biochem. 2006;283:75–83.
35 Steffens S, Veillard NR, Arnaud C, et al. Low dose oral cannabinoid therapy reduces progression of atherosclerosis in mice. Nature. 2005;434:782–786.
36 Jouanjus E, Leymarie F, Tubery M, et al. Cannabis-related hospitalizations: unexpected serious events identified through hospital databases. Br J Clin Pharmacol. 2011;71:758–765.
37 Jouanjus E, Lapeyre-Mestre M, Micallef J; French Association of the Regional Abuse and Dependence Monitoring Centres (CEIP-A) Working Group on Cannabis Complications*. Cannabis use: signal of increasing risk of serious cardiovascular disorders. J Am Heart Assoc. 2014;3:e000638.
39 Mittleman MA, Lewis RA, Maclure M, et al. Triggering myocardial infarction by marijuana. Circulation. 2001;103:2805–2809. Nawrot TS, Perez L, Künzli N, et al. Public health importance of triggers of myocardial infarction: a comparative risk assessment. Lancet. 2011;377:732–740.
40 Mukamal KJ, Maclure M, Muller JE, et al. An exploratory prospective study of marijuana use and mortality following acute myocardial infarction. Am Heart J. 2008;155:465–470.
41 Cecelia P. Johnson-Sasso, David Kao, Lori A. Walker. Marijuana use and short-term outcomes in patients hospitalized for acute myocardial infarction. JACC April 5, 2016, Volume 67, Issue 13
42 Jared P. Reis, PhD, Reto Auer, MD, MAS, Michael P. Bancks, PhD, MPH, David C. Goff Jr, MD, PhD, Cora E. Lewis, MD, MSPH, Mark J. Pletcher, MD, MPH, Jamal S. Rana, MD, PhD, James M. Shikany, DrPH, and Stephen Sidney, MD, MPHAm. Cumulative Lifetime Marijuana Use and Incident Cardiovascular Disease in Middle Age: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. J Public Health. February 16, 2017: e1–e6.
43 Daniel Falkstedt, PhD; Valerie Wolff, MD, PhD; Peter Allebeck, MD, PhD; Tomas Hemmingsson, PhD; Anna-Karin Danielsson, PhD. Cannabis, Tobacco, Alcohol Use, and the Risk of Early Stroke A Population-Based Cohort Study of 45 000 Swedish Men. Stroke. 2017;48:00-00.
44 Rajesh M, Mukhopadhyay P, Batkai S, Patel V, Saito K, Matsumoto S, Kashiwaya Y, Horvath B, Mukhopadhyay B, Becker L, Hasko G, Liaudet L, Wink DA, Veves A, Mechoulam R, Pacher P. Cannabidiol attenuates cardiac dysfunction, oxidative stress, fibrosis, and inflammatory and cell death signaling pathways in diabetic cardiomyopathy. J Am Coll Cardiol 2010;56:2115–2125.
45 Rajesh M, Mukhopadhyay P, Batkai S, Hasko G, Liaudet L, Drel VR, Obrosova IG, Pacher P. Cannabidiol attenuates high glucose-induced endothelial cell inflammatory response and barrier disruption. Am J Physiol Heart Circ Physiol 2007;293:H610–H619.
46 Ruiz-Valdepenas L, Martinez-Orgado JA, Benito C, Millan A, Tolon RM, Romero J. Cannabidiol reduces lipopolysaccharide-induced vascular changes and inflammation in the mouse brain: an intravital microscopy study. J Neuroinflammation 2011;8:5.
47 El-Remessy AB, Al-Shabrawey M, Khalifa Y, Tsai N-T, Caldwell RB, Liou GI. Neuroprotective and blood-retinal barrier-preserving effects of cannabidiol in experimental diabetes. Am J Pathol 2006;168:235–244.
48 Walsh SK, Hepburn CY, Kane KA, Wainwright CL. Acute administration of cannabidiol in vivo suppresses ischaemia-induced cardiac arrhythmias and reduces infarct size when given at reperfusion. Br J Pharmacol 2010;160:1234–1242.
49 Hayakawa K, Mishima K, Irie K, Hazekawa M, Mishima S, Fujioka M, Orito K, Egashira N, Katsurabayashi S, Takasaki K, Iwasaki K, Fujiwara M. Cannabidiol prevents a post-ischemic injury progressively induced by cerebral ischemia via a high-mobility group box1-inhibiting mechanism. Neuropharmacol 2008;55:1280-1286.
50 Hayakawa K, Mishima K, Nozako M, Ogata A, Hazekawa M, Liu AX, Fujioka M, Abe K, Hasebe N, Egashira N, Iwasaki K, Fujiwara M. Repeated treatment with cannabidiol but not Delta9-tetrahydrocannabinol has a neuroprotective effect without the development of tolerance. Neuropharmacol 2007;52:1079–1087.
51 Mishima K, Hayakawa K, Abe K, Ikeda T, Egashira N, Iwasaki K, Fujiwara M. Cannabidiol prevents cerebral infarction via a serotonergic 5-hydroxytryptamine1A receptor-dependent mechanism. Stroke 2005;36:1077–1082.
52 Hayakawa K, Mishima K, Nozako M, Hazekawa M, Irie K, Fujioka M, Orito K, Abe K, Hasebe N, Egashira N, Iwasaki K, Fujiwara M. Delayed treatment with cannabidiol has a cerebroprotective action via a cannabinoid receptor-independent myeloperoxidase-inhibiting mechanism. J Neurochem 2007;102:1488–1496.
53 Christopher P. Stanley, William H. Hind, Cristina Tufarelli, Saoirse E. O’Sullivan; Cannabidiol causes endothelium-dependent vasorelaxation of human mesenteric arteries via CB1 activation. Cardiovasc Res 2015; 107
54 Arackal, B. S., & Benegal, V. (2007). Prevalence of sexual dysfunction in male subjects with alcohol dependence. Indian Journal of Psychiatry, 49(2), 109.
55 Ida Maiorino, M. (2014). Diabetes and sexual dysfunction: current perspectives.
56 Breyer, B. N., Cohen, B. E., Bertenthal, D., Rosen, R. C., Neylan, T. C., & Seal, K. H. (2014). Sexual dysfunction in male Iraq and Afghanistan war veterans: Association with posttraumatic stress disorder and other combat‐related mental health disorders: A population‐based cohort study. The journal of sexual medicine, 11(1), 75-83.
57 Mirone V, Ricci E, Gentile V, Basile Fasolo C, Parazzini F. Determinants of erectile dysfunction risk in a large series of Italian men attending andrology clinics. Eur Urol. 2004;45:87–91.
58 Van Thiel DH, Lester R. The effect of chronic alcohol abuse on sexual function. th Clin Endocrinol Metab. 1979;8:499–510.
59 Grover, S., Mattoo, S. K., Pendharkar, S., & Kandappan, V. (2014). Sexual dysfunction in patients with alcohol and opioid dependence. Indian journal of psychological medicine, 36(4), 355.
60 Gerra, G., Manfredini, M., Somaini, L., Maremmani, I., Leonardi, C., & Donnini, C. (2016). Sexual dysfunction in men receiving methadone maintenance treatment: Clinical history and psychobiological correlates. European addiction research, 22(3), 163-175.
61 Yee, A., Loh, H. S., & Ng, C. G. (2014). The prevalence of sexual dysfunction among male patients on methadone and buprenorphine treatments: a meta‐analysis study. The journal of sexual medicine, 11(1), 22-32.
62 (McVary KT, Carrier S, Wessles H et al. Smoking and erectile dysfunction: evidence based analysis. J Urol. 2001; 166:1624—32.
63 Feldman HA, Goldstein I, Hatzichristou DG et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994; 151:54—61.
64 Mannino DM, Klevens RM, Flanders WD. Cigarette smoking: an independent risk factor for impotence? Am J Epidemiol. 1994; 140:1003—8.
65 Spangler JG, Summerson JH, Bell R et al. Cigarette smoking and erectile dysfunction. J Fam Pract. 2002; 51:81. Letter.
66 Tengs TO, Osgood ND. The link between smoking and impotence: two decades of evidence. Prev Med. 2001; 32:447—52.
67 Condra M, Morales A, Owen JA et al. Prevalence and significance of tobacco smoking in impotence. Urology. 1986; 27:495—8.
68 Gades NM, Nehra A, Jacobson DJ et al. Association between smoking and erectile dysfunction: a population-based study. Am J Epidemiol. 2005; 161:346—51.
69 Natali A, Mondaini N, Lombardi G et al. Heavy smoking is an important risk factor for erectile dysfunction in young men. Int J Impot Res. 2005; 17:227—30.
70 Austoni E, Mirone V, Parazzini F et al. Smoking as a risk factor for erectile dysfunction: data from the Andrology Prevention Weeks 2001—2002. A study of the Italian Society of Andrology (S.I.A.). Eur Urol. 2005; 48:810—8.
71 Rosen MP, Greenfield AJ, Walker TG et al. Cigarette smoking: an independent risk factor for atherosclerosis in the hypogastric-cavernous arterial bed of men with arteriogenic impotence. J Urol. 1991; 145:759—63.
72 Shiri R, Hakama M, Hakkinen J et al. Relationship between smoking and erectile dysfunction. Int J Impot Res. 2005; 17:164—9.
73 Polsky JY, Aronson KJ, Heaton JP et al. Smoking and other lifestyle factors in relation to erectile dysfunction. BJU Int. 2005; 96:1355—9.
74 Park K, Ku JH, Kim SW et al. Risk factors in predicting a poor response to sildenafil citrate in elderly men with erectile dysfunction. BJU Int. 2005; 95:366–70.
75 Dishy V, Harris PA, Pierce R et al. Sil denafil does not improve nitric oxide-mediated endothelium-dependent vascular responses in smokers. Br J Clin Pharmacol. 2004; 57:209—12.
76 Derby CA, Mohr BA, Goldstein I et al. Modifiable risk factors and erectile dysfunction: can lifestyle changes modify risk? Urology. 2000; 56:302—6.
77 Guay AT, Perez JB, Heatley GJ. Cessation of smoking rapidly decreases erectile dysfunction. Endocr Pract. 1998; 4:23—6.
78 Pourmand G, Alidaee MR, Rasuli S et al. Do cigarette smokers with erectile dysfunction benefit from stopping?: a prospective study. BJU Int. 2004; 94:1310—3.
79 Androvicova, R., et al. “Endocannabinoid system in sexual motivational processes: Is it a novel therapeutic horizon?.” Pharmacological research 115 (2016): 200.
80 Androvicova, R., Horacek, J., Tintera, J. et al.Individual prolactin reactivity modulates response of nucleus accumbens to erotic stimuli during acute cannabis intoxication: an fMRI pilot study. Psychopharmacology (2017)
81 Centers for Disease Control and Prevention (CDC). Alcohol and Public Health: Alcohol-Related Disease Impact (ARDI). Average for United States 2006–2010 Alcohol-Attributable Deaths Due to Excessive Alcohol Use. Available at: https://nccd.cdc.gov/DPH_ARDI/Default/Report.aspx?T=AAM&P=f6d7eda7-036e-….
82 World Health Organization (WHO). Global Status Report on Alcohol and Health. p. XIV. 2014 ed. Available at: http://www.who.int/substance_abuse/publications/global_alcohol_report/ms…
83 U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014
84 Gable, Robert S., “The Toxicity of Recreational Drugs,” American Scientist (Research Triangle Park, NC: Sigma Xi, The Scientific Research Society, May-June 2006) Vol. 94, No. 3, p. 207.
85 Lachenmeier DW, Rehm J. Comparative risk assessment of alcohol, tobacco, cannabis and other illicit drugs using the margin of exposure approach. Scientific Reports. 2015;5:8126.
Kannabia Seeds Company sells to its customers a product collection, a souvenir. We cannot and we shall not give growing advice since our product is not intended for this purpose.
Kannabia accept no responsibility for any illegal use made by third parties of information published. The cultivation of cannabis for personal consumption is an activity subject to legal restrictions that vary from state to state. We recommend consultation of the legislation in force in your country of residence to avoid participation in any illegal activity.

Vienna hosts the 9th edition of the Cultiva Hanfmesse, one of the most important cannabis fairs in Europe, held from 7 to 9 October in Vösendorf Eventpyramid. Professionals will be spread over 140 exhibitors, where attendees will ...
There are more than 100 different cannabinoids known to science; and many more are being discovered as the expansion of marijuana research continues. As new terms are introduced into our lexicon, you ...








Kannabia Seed Company sells its customers hobby (collection) seeds for personal use. Its germination and cultivation is prohibited. The buyer undertakes to consult the legislation in force in his country of residence to avoid incurring in the performance of an illegal activity.
 Fast free shipping
Fast free shipping Iberian Peninsula express shipping
0€ Orders over 60€
*6€ orders under 59€
East, West, South Europe express shipping
0€ Orders over 150€
*18€ orders under 149€
North Europe express shipping
0€ Orders over 160€
*20€ orders under 159€
Ireland, Norway, UK normal shipping
0€ Orders over 60€
*6€ orders under 59€
Rest of the world normal shipping
0€ Orders over 180€
*25€ orders under 179€
Shipping costs can be confirmed in your shopping cart.
For additional shipping methods, please reach out through info@kannabia.com.
 Coupons
Coupons 

*Your coupon will be sent via email.
 Customer support
Customer support 
*Should you have any question, comment or feedback, please do not hesitate to contact us.






 Secure Payment
Secure Payment 

 Credit card
Credit card Bank transfer
Bank transfer Cash on delivery**
Cash on delivery**